Thyroid Cancer Lymph Nodes: Symptoms, Diagnosis, Treatment, and Prognosis Explained
When discussing thyroid cancer, one of the most important concerns for patients and families is the involvement of thyroid cancer lymph nodes. The spread of cancer cells to nearby lymph nodes is common in certain types of thyroid cancer and can influence treatment decisions and long-term outcomes. Understanding how and why this happens empowers you to make informed healthcare choices.
Although lymph node involvement may sound alarming, it does not always mean a poor prognosis. In fact, many patients with thyroid cancer lymph nodes involvement, especially in early stages, experience excellent survival rates with proper management. This comprehensive guide explains everything you need to know, from symptoms and diagnosis to treatment options and the latest research developments.
Overview
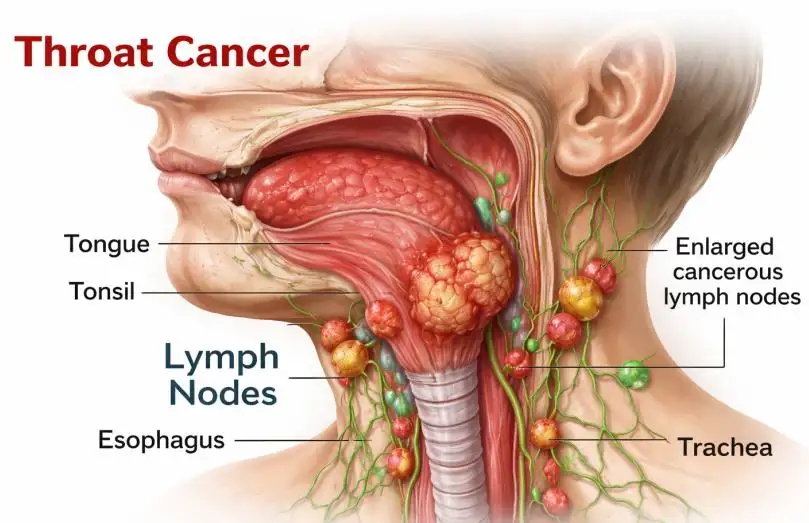
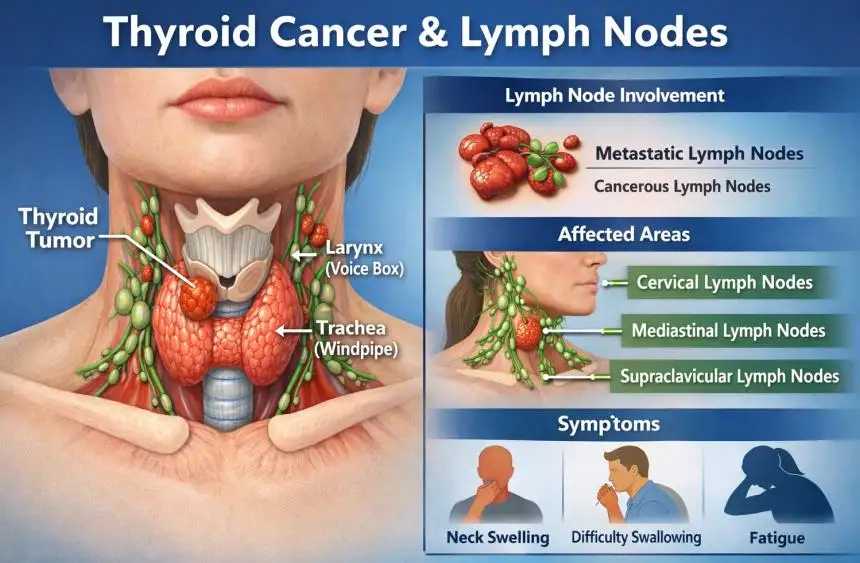
The thyroid is a butterfly-shaped gland located at the front of the neck. Thyroid cancer develops when abnormal cells grow uncontrollably within this gland. In some cases, cancer cells spread beyond the thyroid to nearby lymph nodes in the neck.
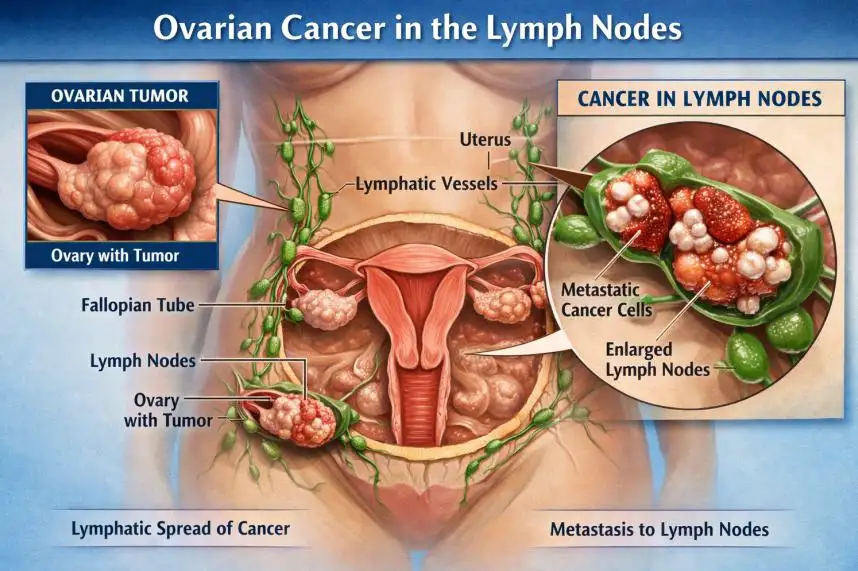
Lymph nodes are small, bean-shaped structures that play a key role in the immune system. When thyroid cancer spreads to these nodes, it is known as lymph node metastasis. This process is most frequently associated with differentiated thyroid cancers.
According to the American Cancer Society, lymph node involvement is particularly common in papillary thyroid cancer, yet survival outcomes remain highly favorable in most patients.
Types
There are several types of thyroid cancer, and each carries a different likelihood of lymph node spread.
| Type of Thyroid Cancer | Likelihood of Lymph Node Involvement | Typical Behavior |
|---|---|---|
| Papillary Thyroid Cancer | High (up to 30–80%) | Slow-growing, often spreads to neck lymph nodes |
| Follicular Thyroid Cancer | Lower | More likely to spread through bloodstream |
| Medullary Thyroid Cancer | Moderate | May spread to lymph nodes early |
| Anaplastic Thyroid Cancer | Variable but aggressive | Rapid growth and distant spread |
Papillary thyroid cancer is the most common type and frequently presents with thyroid cancer lymph nodes enlargement at diagnosis.
Causes and Risk Factors
The exact cause of thyroid cancer remains unclear, but several risk factors increase the likelihood of both thyroid cancer and lymph node spread:
-
Exposure to radiation, especially during childhood
-
Family history of thyroid cancer
-
Genetic mutations (e.g., RET mutations in medullary thyroid cancer)
-
Female gender
-
Age (younger patients more commonly show lymph node involvement in papillary type)
Certain genetic syndromes, such as Multiple Endocrine Neoplasia (MEN), increase the risk of medullary thyroid cancer, which may spread to lymph nodes early.
Symptoms and Early Warning Signs
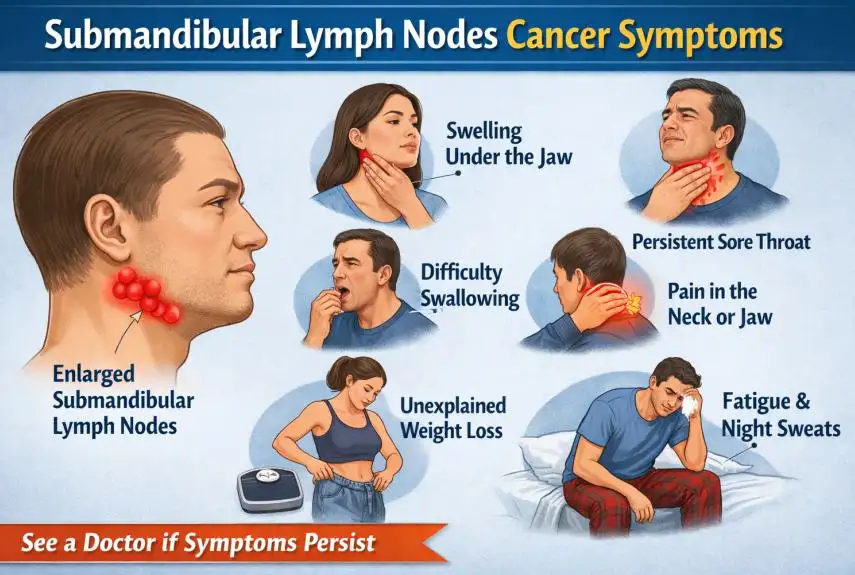
Thyroid cancer lymph nodes involvement may produce noticeable symptoms, although some patients remain asymptomatic.
Common warning signs include:
-
A painless lump in the neck
-
Enlarged lymph nodes that feel firm and persistent
-
Hoarseness or voice changes
-
Difficulty swallowing
-
Persistent cough not related to a cold
-
Neck discomfort
In many cases, enlarged lymph nodes are discovered during routine imaging rather than through physical symptoms.
Diagnosis
Accurate diagnosis is essential for determining the extent of thyroid cancer lymph nodes involvement.
Common diagnostic methods include:
| Diagnostic Tool | Purpose |
|---|---|
| Neck Ultrasound | Detects thyroid nodules and enlarged lymph nodes |
| Fine-Needle Aspiration (FNA) Biopsy | Confirms cancer in thyroid or lymph nodes |
| CT or MRI Scan | Evaluates spread beyond the thyroid |
| Thyroglobulin Testing | Monitors recurrence after treatment |
| PET Scan | Used in advanced or recurrent cases |
Ultrasound-guided biopsy is particularly valuable in identifying cancerous lymph nodes before surgery.
Treatment Options
Treatment depends on the type of thyroid cancer, the number of lymph nodes involved, and whether the cancer has spread beyond the neck.
Surgery
Surgery is the primary treatment and may include:
-
Total thyroidectomy (removal of the thyroid gland)
-
Central neck dissection (removal of affected lymph nodes)
-
Lateral neck dissection (if cancer has spread further)
Radioactive Iodine Therapy
Radioactive iodine (RAI) is commonly used after surgery in differentiated thyroid cancers to destroy remaining cancer cells.
Targeted Therapy
In advanced or resistant cases, targeted therapies may be prescribed. The National Cancer Institute highlights the use of kinase inhibitors for certain progressive thyroid cancers.
External Beam Radiation and Chemotherapy
These are less common but may be considered in aggressive or inoperable cases.
Prevention and Lifestyle Recommendations
While thyroid cancer cannot always be prevented, certain measures may reduce risk or support recovery:
-
Avoid unnecessary radiation exposure
-
Maintain regular medical checkups if at high risk
-
Follow thyroid hormone therapy precisely after surgery
-
Eat a balanced diet rich in iodine (unless restricted during RAI preparation)
-
Stay physically active to support overall immune health
Patients with genetic risk factors may benefit from early screening and genetic counseling.
Prognosis and Survival Rates
One reassuring fact about thyroid cancer lymph nodes involvement is that prognosis remains excellent in most cases—particularly for papillary thyroid cancer.
| Condition | 5-Year Survival Rate |
|---|---|
| Localized Thyroid Cancer | Over 99% |
| Regional (Lymph Node Spread) | Approximately 98% |
| Distant Metastasis | Around 55–75% |
Younger patients generally have better outcomes, even when lymph nodes are affected. Early detection and appropriate treatment significantly improve long-term survival.
Latest Research and Innovations
Advancements in thyroid cancer research continue to improve patient outcomes.
Emerging innovations include:
-
Molecular testing to predict aggressive behavior
-
Personalized targeted therapies
-
Minimally invasive surgical techniques
-
Improved imaging technologies for detecting small lymph node metastases
Institutions supported by the American Thyroid Association are actively developing updated guidelines for managing thyroid cancer lymph nodes more effectively.
Coping and Support for Patients
A diagnosis involving thyroid cancer lymph nodes can feel overwhelming, but support is available.
Helpful strategies include:
-
Joining thyroid cancer support groups
-
Speaking openly with your healthcare team
-
Seeking counseling for emotional well-being
-
Connecting with survivor networks
-
Staying informed about your condition
Emotional health plays a crucial role in recovery. Many patients find reassurance in understanding that lymph node involvement does not automatically mean a poor outcome.
Conclusion
Thyroid cancer lymph nodes involvement is common, particularly in papillary thyroid cancer, but it does not necessarily indicate a life-threatening situation. With modern surgical techniques, radioactive iodine therapy, and targeted treatments, the majority of patients achieve excellent long-term survival.
Early diagnosis, personalized treatment, and ongoing monitoring are key to successful outcomes. If you or a loved one is facing thyroid cancer, remember that medical advancements continue to improve care and prognosis every year.
FAQ
1. Does thyroid cancer spreading to lymph nodes mean stage 4?
No. Lymph node involvement usually represents regional spread (often Stage III or earlier, depending on age and tumor size), not necessarily Stage IV.
2. Can thyroid cancer lymph nodes be cured?
Yes. In many cases, surgical removal combined with radioactive iodine therapy can successfully eliminate cancer from lymph nodes.
3. Are swollen lymph nodes always cancerous?
No. Lymph nodes can enlarge due to infections or inflammation. A biopsy is required for confirmation.
4. How often does papillary thyroid cancer spread to lymph nodes?
It can occur in 30–80% of cases, especially in younger patients.
5. Is lymph node removal dangerous?
Neck dissection is generally safe when performed by experienced surgeons, though risks include nerve injury and calcium imbalance.